Post-auricular Muscle Artifact In BAER
This is a question that I got about post-auricular muscle artifact on intraoperative brainstem auditory responses. These are one of those responses that I don’t have any of my own images because I’ve never seen it live. This is due to the fact that I have never placed my A1 or A2 recording electrodes behind the ear, which is the cause of the artifact overlapping the middle latency responses.
I doubt many people have been fooled by this in the OR, so it isn’t something that gets a lot of attention when training someone on brainstem auditory evoked potentials. But it does end up making its rounds on as questions on the CNIM and DABNM examination.
But before I go into a more detailed, let me help direct others that might have similar questions.
The Neuromonitoring Forum
One area of the website that I would really encourage readers of this blog to spend some time and effort on is the neuromonitoring forum. I think it opens up a lot more possibilities than someone just asking me for a one-on-one response to a question. I gave an answer to the question (see below), but maybe there is another angle to cover that I didn’t consider. That’s where the neuromonitoring forum comes in. The way I see it, the forum can serve 3 major purposes.
- Provide answers to those that have questions. Throughout my entire career, I’ve always made sure to work for a company that had people on staff that are leaders in the field. The easiest way to fast track your own learning is by gaining knowledge from others. I understand that not everyone has been as fortunate. For those without that perk, the forum is the place to be. Ask questions and follow up.
- Give a platform for leaders to emerge. It takes some guts to stick your neck out there just to help others. But trust me, people are looking. This is a great opportunity to help yourself by helping others first.
- Join the club. The IONM community is pretty small. Less than 3700 CNIM and 200 DABNM as I write this. You can become acquaintances and friends pretty fast with a good percentage of the field. This is an excellent place to network.
I get questions all the time from people I’ve met along the way. Phone calls, text, emails, live chats, etc. I’ve tried my best to give a complete and correct answer every time. But it is a lot of effort, so I’d like to leverage the content a little bit for all to see. If you do ask me a question, chances are I will ask you to put it on the forum, or it will land here as a blog post.
That way you have a better chance of getting a better answer. Plus, someone else is or will be wondering the same exact thing.
Here’s a question that I had sitting in my archives:
The Question
Feel free to share this with others in our group.
I was reading about ABR and I came across the following topic: Post-auricular Myogenic response and Middle latency potential.
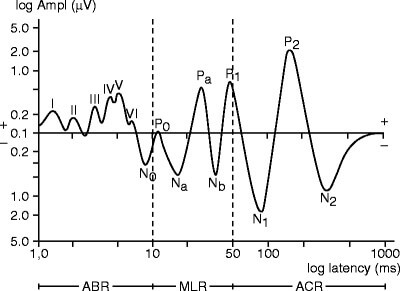
The latency that we would expect to see them:
Postauricular – 13/20 msec
Middle auditory – 12/50 msec
Here are my questions:
1. What is the very large amplitude potential following the ABR waves I-V at approximately 15ms?
Post-auricular myogenic artifact or Middle latency potential?
Usually, the post-auricular myogenic artifact or post-auricular muscle activity may appear toward the end of ABR waveform if an analysis time of 15msec or longer is used.
2. When should I expect to find that response? Between 13-20msec range?
3. Does it appear on both sides or just on the ipsilateral side?
4. Are both of these responses from the upper brainstem?
5. How can I differentiate between a middle auditory response and a post-auricular myogenic artifact?
My response:
In the OR, we only monitor short latency ABR responses, the wave I, III and V that you are used to seeing. The reason that you’re not used to even seeing these on the screen in the case you’ve been on is because we use a pretty short time base. I start out with a 15 ms window and place my markers. It can also be useful to change the time base to 10ms total in order to better see subtle shifts in latency. You should start with 15 ms at least just to verify that you are marking the correct waves.
These middle latency potentials are upper brainstem/reticular/thalamic potentials that are unreliable in the OR but are used by an audiologist in clinical settings.
Post-auricular Muscle Artifact
The post-auricular muscle (or PAM) can cause a post-auricular myogenic response (also called post-auricular muscle artifact, or PAMR), which is artifact picked up by the recording electrodes (in additions to these middle latency cortical potentials) from muscle activity that distorts the amplitudes and latencies of these middle latency potentials, as well as the short latency response we are analyzing.
They are seen when you place your recording electrode behind the ear or near the neck, which is why we put our recording electrodes pre-auricular for all BAER cases. The 2 places that I’ve had success is just anterior to the tragus and just below the tragus near the ear lobe insertion. I typically start anterior to the tragus, mostly because this seems to be a more common electrode placement. If I am not satisfied with wave I collection from the Ai-Cz montage, I may test out the second position. I do this because wave I of the brainstem auditory evoked potentials are near-field responses. This will sometimes reproduce a better wave I response without any post-auricular muscle artifact.
The PAM artifact is known for its large amplitudes and to be intermittent (since it depends on the muscle contraction to cause the artifact, which could be ipsilateral, contralateral, or bilateral).
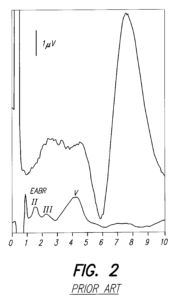
On the CNIM or DABNM written exam, if there was a picture of ABRs with huge amplitudes (you can tell by looking at the display gain used on the picture, or the size of the waves I-V, which are very small (0.2-0.5uV), I would be thinking PAM even before I looked at the answers to choose from. The latencies you stated in the question are good ranges to know for the artifact and the middle latency responses.
To make sure that you understand the information and can put it to practical use, please answer the question below.
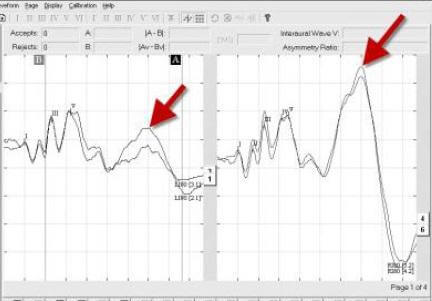
Guess which one of the 2 traces has the muscle artifact…
PRO TIP – Beyond what’s listed above, I don’t think I would spend too much more time on middle latency or late latency ABRs. Your time studying for the CNIM or DABNM test would be better suited elsewhere.
In that same image (the trace without the PAM), what can you comment on about the absolute latencies of Wave II, III and V compared to what you might see in an acoustic neuroma case in the OR, and what might you attribute this to? Please leave your responses in the comments section.

Joe Hartman
Joe came into the neuromonitoring field as a board-certified chiropractic neurologist with an interest in neurodiagnostics. After earning a diplomate from the American Board of Neurophysiologic Monitoring, he started IntraoperativeNeuromonitoring.com as a resource for other surgical neurophysiologist looking to learn and discuss all things neuromonitoring. He spends more time tinkering on this website in his spare time than he cares to admit.
Subscribe to our Awesome Newsletter.
3 Comments
Keep Learning
Here are some related guides and posts that you might enjoy next.

How To Have Deep Dive Neuromonitoring Conversations That Pays Off…
How To Have A Neuromonitoring Discussion One of the reasons for starting this website was to make sure I was part of the neuromonitoring conversation. It was a decision I made early in my career... and I'm glad I did. Hearing the different perspectives and experiences...

Intraoperative EMG: Referential or Bipolar?
Recording Electrodes For EMG in the Operating Room: Referential or Bipolar? If your IONM manager walked into the OR in the middle of your case, took a look at your intraoperative EMG traces and started questioning your setup, could you defend yourself? I try to do...

BAER During MVD Surgery: A New Protocol?
BAER (Brainstem Auditory Evoked Potentials) During Microvascular Decompression Surgery You might remember when I was complaining about using ABR in the operating room and how to adjust the click polarity to help obtain a more reliable BAER. But my first gripe, having...
Bye-Bye Neuromonitoring Forum
Goodbye To The Neuromonitoring Forum One area of the website that I thought had the most potential to be an asset for the IONM community was the neuromonitoring forum. But it has been several months now and it is still a complete ghost town. I'm honestly not too...

EMG Nerve Monitoring During Minimally Invasive Fusion of the Sacroiliac Joint
Minimally Invasive Fusion of the Sacroiliac Joint Using EMG Nerve Monitoring EMG nerve monitoring in lumbar surgery makes up a large percentage of cases monitored every year. Using EMG nerve monitoring during SI joint fusions seems to be less utilized, even though the...

Physical Exam Scope Of Practice For The Surgical Neurophysiologist
SNP's Performing A Physical Exam: Who Should Do It And Who Shouldn't... Before any case is monitored, all pertinent patient history, signs, symptoms, physical exam findings and diagnostics should be gathered, documented and relayed to any oversight physician that may...

Wave II, III and V would be delayed in absolute latencies with normal interpeak conduction time between III to V. You may or may not have a Wave I and an ECOG would be helpful along with the possible need of a facial free running/ triggered 7th nerve on the same side as the acoustic.
Thank you, Rhonda.
I would really push for that CN 7 monitoring in these cases. IONM does a great job here and has a ton of literature to back the clinical usefulness.
I agree, thank you.