by Joe Hartman | Feb 25, 2013 | Neuromonitoring Training
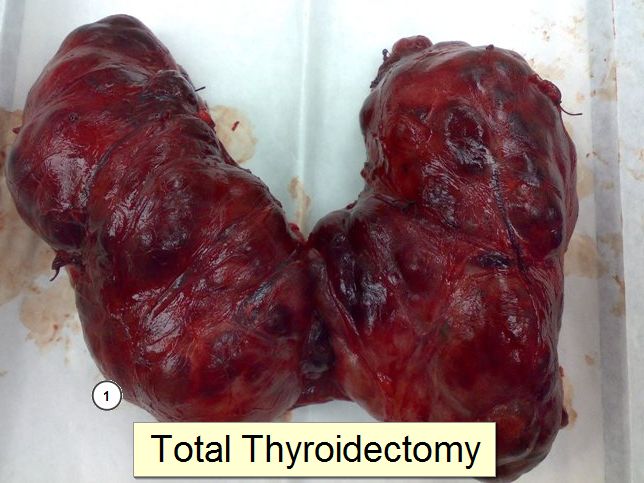
Triggered EMG for Total Thyroidectomy In one of my previous post, I wrote about monitoring the recurrent laryngeal nerve with triggered EMG and the possibility of giving the surgeon misinformation. That misinformation (in that hypothetical scenario) could lead the... 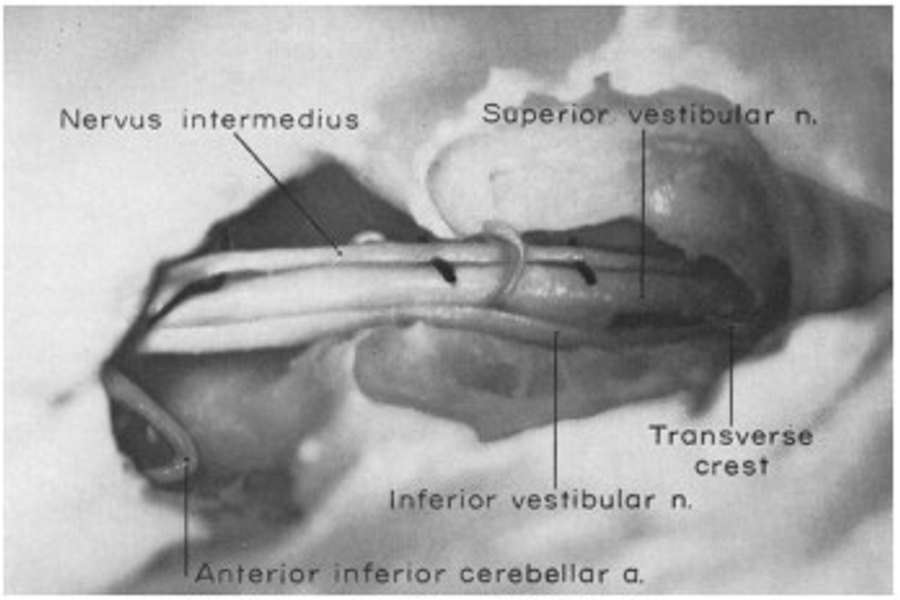
by Joe Hartman | Feb 18, 2013 | Neuromonitoring Training
Possible Facial Nerve Monitoring Blunder… Facial nerve monitoring is one of the things that we as intraoperative neurophysiologist can perform with a high level of certainty Because of the amount of research demonstrating its usefulness, the information we give... 
by Joe Hartman | Feb 13, 2013 | IOM Jobs, Neuromonitoring Training
Land Your First IOM Job It’s the weirdest thing… IOM companies are always looking to hire someone with at least a CNIM and 3 years experience while so many people are always wondering where to find their first IOM job. There’s always that... 
by Joe Hartman | Feb 6, 2013 | Neuromonitoring Training
I came across some papers on motor evoked potentials (MEPs) that got me thinking a little bit. It got me thinking about small influences in the operating room that may, or may not, affect our tracings during our cases. Specifically, MEPs. Here’re some snippets... 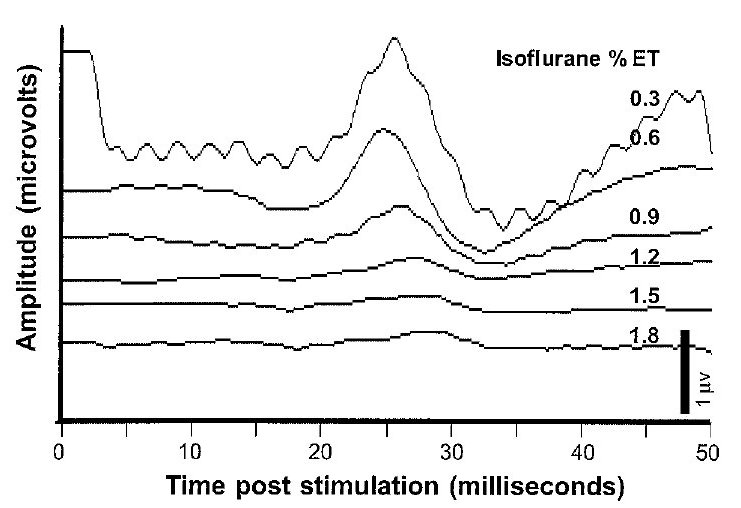
by Joe Hartman | Oct 29, 2012 | Neuromonitoring Training
SSEP Baseline One of the few things in IONM that’s agreed upon (well, mostly anyways), is that an amplitude reduction of 50% in SSEP baseline, or a 10% latency shift off of those somatosensory evoked potential baselines, is a reliable alarm criterion to use... 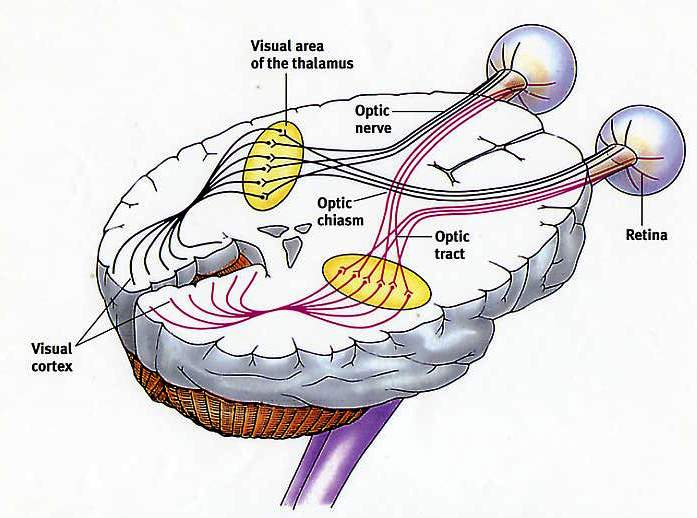
by Joe Hartman | Oct 24, 2012 | Neuromonitoring Training
When talking about intraoperative monitoring of visual evoked potentials, it’s almost like you’re getting a history lesson, seeing as most groups aren’t doing them. And most have 2 things that come to mind right away. First, visual evoked potentials...