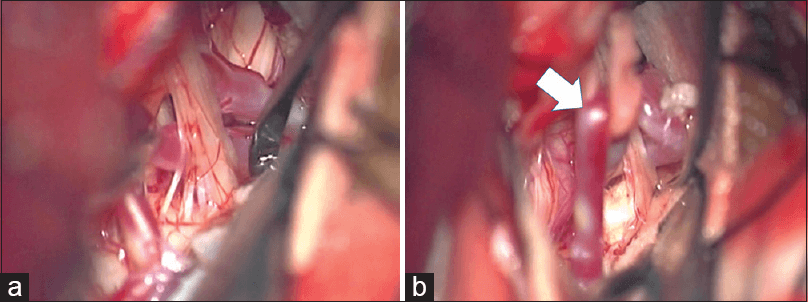
BAER (Brainstem Auditory Evoked Potentials) During Microvascular Decompression Surgery
You might remember when I was complaining about using ABR in the operating room and how to adjust the click polarity to help obtain a more reliable BAER. But my first gripe, having a big honking tumor pressing up against the nerve, isn’t a problem in MVD surgery. The other problems revolving around the waves being small and susceptible to noise from a hostile electrical environment (the operating room) and larger physiologic responses (EEG).
But there is a new paper out by Joo et. al. that might help address this problem.
The Search To Make BAER Better
Because of the poor signal-to-noise ratio of BAER, we have been forced to collect thousands of sweeps in order to get a reliable response. During that collection period, even small disturbances could severely distort the responses collected up to that point. So not only is there a long collection period, clearing out traces and starting over isn’t something uncommon.
The Rep Rate
So faster collection rates would be more favorable. Joo looked at the collection of BAER using rep rates of 10 to 100 Hz, going up by 10 Hz. They looked for the sweet spot where there was still a reliable wave V collected as fast as possible. They found that between 40-50 Hz had reliable waves without surgical artifact. They then came up with 43.9 Hz as their “go to” rate to better avoid overlap with common noise frequencies.
The Sweeps
They then looked at the necessary number of sweeps in order to record a reliable response. They found that 400 traces was as reliable as 1000 traces. Some quick math (400/43.9) shows that they were able to collect a reliable BAER in 9.11 seconds, or about 6 every minute.
What’s The Up Side?
Reducing time to collect is always a good thing. I can think of 4 ways this is very helpful:
- You’re able to identify problems faster
- You’re able to verify that it isn’t technical faster
- You’re better able to collect in between use of the bovie
- You’re less likely to have to clear out a trace and start all over
What’s The Catch?
But there has to be something more to the story, right? I mean who hasn’t already considered just turning up the rep rate for faster collection?
The last part of their study was to compare amplitude change in wave V > 50% vs. changes in interpeak latency of > 1.0 ms. Their outcomes showed that it was only the change in wave V that was useful, although a shift and latency may also be seen.
That changes things a little bit. If only amplitude change of wave V is significant, then we might elect to give up good looking waves I and III, as well as appropriate interpeak latencies in order to have a reliable wave V at a collection speed that allows for faster observation of changes. Most people are hesitant to go above a rep rate of 20 Hz because of it can distort waveform, but staying below 50 Hz is not a new suggestion either.
- This technique was used on patients without hearing problems. I would not carry this over to acoustic neuroma cases, where you might already battling with poor waveforms. Increasing the rep rate and lowering the sweeps this much might make any data collection impossible.
- This protocol is still new. It looks like obtaining their objective (a reliable wave V) is doable, but I’d like to see more cases with changes in order to call this a superior technique.
- I would like to see a larger sample of patients with changes before abandoning looking at interpeak latency as something that should be reported to the surgeon. I’ve always felt that amplitude changes are a better marker than latency changes, but I have seen a latency shift only with almost no amplitude change have post op deficits. This was with SSEPs, but enough reason for me to continue to use latency changes as something that needs to be looked at.

Joe Hartman
Subscribe to our Awesome Newsletter.
2 Comments
Keep Learning
Here are some related guides and posts that you might enjoy next.

How To Have Deep Dive Neuromonitoring Conversations That Pays Off…
How To Have A Neuromonitoring Discussion One of the reasons for starting this website was to make sure I was part of the neuromonitoring conversation. It was a decision I made early in my career... and I'm glad I did. Hearing the different perspectives and experiences...

Intraoperative EMG: Referential or Bipolar?
Recording Electrodes For EMG in the Operating Room: Referential or Bipolar? If your IONM manager walked into the OR in the middle of your case, took a look at your intraoperative EMG traces and started questioning your setup, could you defend yourself? I try to do...
Bye-Bye Neuromonitoring Forum
Goodbye To The Neuromonitoring Forum One area of the website that I thought had the most potential to be an asset for the IONM community was the neuromonitoring forum. But it has been several months now and it is still a complete ghost town. I'm honestly not too...

EMG Nerve Monitoring During Minimally Invasive Fusion of the Sacroiliac Joint
Minimally Invasive Fusion of the Sacroiliac Joint Using EMG Nerve Monitoring EMG nerve monitoring in lumbar surgery makes up a large percentage of cases monitored every year. Using EMG nerve monitoring during SI joint fusions seems to be less utilized, even though the...

Physical Exam Scope Of Practice For The Surgical Neurophysiologist
SNP's Performing A Physical Exam: Who Should Do It And Who Shouldn't... Before any case is monitored, all pertinent patient history, signs, symptoms, physical exam findings and diagnostics should be gathered, documented and relayed to any oversight physician that may...
MEP Loss With Levetiracetam: Another Anesthetic To Consider With Motor Evoked Potentials
Levetiracetam And Its Effects On Transcranial Motor Evoked Potentials During Surgery Levetiracetam (AKA Keppra) It's pretty widely accepted that inhalational agents and muscle relaxants will reduce the effectiveness of transcranial motor evoked potentials during...

Hello.
Do you know about the monitoring machine to recording BAEP in this paper.
Because, our monitoring machine can’t take this one equally.
Signal distorting is more awaken.
Our machine is Nim-eclipse.
Xltek Protektor