CNIM Exam Preparation: Far-Field Responses
I’ve asked a couple of readers what they were having trouble with when preparing for the CNIM exam. In the last post, I went over when to use constant voltage and constant current. This time, I’m going to go over far-field potentials and how those are formed.
Near-Field vs. Far-Field
Near-field potentials are pretty easy to understand. You just put your recording electrode as close to the generator point as possible. If you want a nice N20, you stick a needle in the contralateral head from the wrist you’re stimulating. You wouldn’t want to stick it in the shoulder because that’s not where you want to record over. Consider yourself lucky to get any kind of reliable response with that poor setup. Needle placement is especially important when recording a near-field response (HINT: possible CNIM exam question there).
But far-field potentials aren’t the same. There are a couple principals of conducting electric current through the body and recording a wave that you need to understand before you’ll fully grasp it.
List of Far-Field Potentials You Need To Know For The CNIM Exam
When you go to take the CNIM or DABNM written exam, you need to have an understanding of how to generate a far-field potential to better figure out if a response is a near-field or far-field response. But you need to also have a list of those memorized, like this one here…
- P14 UE SSEP
- N18 UE SSEP
- P31 LE SSEP
- N34 LE SSEP
- Wave III ABR
- Wave V ABR
But you need to really understand why these are far-field responses. And here’s a hint…
It’s not because they are a specific distance from the recording site.
There is no such distance that distinguishes a near-field from a far-field response… that’s too easy.
First off, far-field responses have a larger spread than near-field responses. You will equally record the same generator from various distances.
How is that possible?
Because we’re not just recording electrical impulse carried through a nerve or tract. Electrical current transmits through any solution that has high enough sodium levels (just like in your middle school science project).
Our body’s tissue is able to conduct these electric currents because our tissues, blood, CSF, etc.
Here’s an example… the EKG artifact that you pick up on EEG recordings. The electrical current is created in the heart, but it’s not transmitted through some tract directly from the heart to the brain (cardiospinal tract?). The current flows through the tissue in the body and gets picked up by the head electrodes.
Creation of electric current from all over occurs. Luckily, it follows some rules to manage the chaos.
3 principals that electric current follow
- If resistance is equal, the current will flow evenly in all directions.
- The current will always take the path of least resistance.
- The amplitude varies by the square of the distance between the recording electrode from the generator… the closer the recording electrode, the bigger the amplitude.
Now that you know what kind of current acts on the generator points, and the rules that this current follows, you’ree able to understand why far-field potentials recorded from a wide area (and near-field in a small area), why some areas are better to record from than others, why these various recording sites are not always the same in amplitude and why it is theoretically possible to record any potential from anywhere on the body.
In order to benefit from this, we need to utilize this information to give us a clue as to what’s going on and where. We need to record from areas that are strong enough to give reproducible signals, along areas of interest. These are called the generator points.
Generator points
The generator points are the areas believed to give off strong enough signals to create a reliable waveform. Most generator points are approximations (pretty much a guess) as to exactly where or how this signal is being created.
And now that you understand that the generator points are not created just by activation of a nerve, you’ll appreciate the possibilities of what it is that we are actually recording. Here’s what is currently accepted as the actual source of evoked potentials.
- activity from a cluster of sensory neurons (for example, the N13 cervical response has a larger amplitude over the C5 segment than the C2 spinal segment. That means that this is a near-field response, with the active electrode over the sensory neurons)
- synaptic activity between neurons (for example, the P100 response in VEP are from cortical activity from light stimulation)
- AP along axons (for example, when stimulating over the brachial plexus or popliteal fossa, move your electrode along the nerve and still get a very similar response in amplitude size, with a different latency. This traveling response is a good example of generating the potential along the nerve axon)
- Non-neural events, like a change in direction of a tract, or a change in the compartment that houses that neural structure (for example, as the P14 SSEP response comes from a changes direction after entering the foramen magnum)
- Volume conduction, or electrical current through the conduction through the body (for example, Wave I BAER is considered a near-field response because even small changes in the distance of the Ai electrode (Cz-Ai montage) will decrease the amplitude. However, the Cz reference electrode also active and gives off a far-field potential at far distances. It has a large spread or distribution)
And this does not happen in isolation. That’s why Wave I of BAER has both near-field and far-field potentials (but if I had to guess one or the other on the CNIM or DABNM, I would put it as near-field).
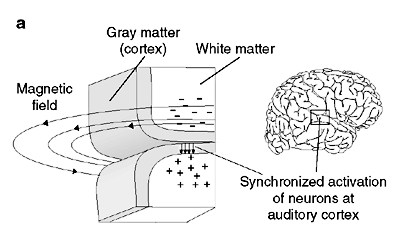
Image from http://bit.ly/10SIorvPositive vs. Negative?
A wave will either have a peak or a trough for you to put your markers on. How that is determined is the relationship of your active and reference electrodes and the polarity of the electric current. That polarity is determined by the orientation of the dipole.
Dipole
A dipole is a pair of electric charges or magnetic poles, of equal magnitude but of opposite sign or polarity, separated by a small distance. So on one side you have a positive charge, and on the other you have a negative charge. This dipole takes different paths, some being horizontal and some vertical. With the round cortex with sulcus causing a 90-degree change in tissue orientation, you will see how recording electrodes are influenced by various electrical sources, from various distances, with various polarities. Some of these potentials are additive, others will cancel out the potentials.

The dipole helps explain why a wave is positive or negative, depending on the area the recording electrodes are placed. For example, the N13 cervical response is a near-field, horizontal dipole. That means that the active electrode placed on the posterior neck will result in a negative peak while placement over the anterior neck will result in a positive valley.
The dipoles determine the polarity of the potential in relationship to where your active and reference electrodes are placed.
Far-Field Potentials Final Verdict
Now you see why far-field potentials are a little tricky, thanks to volume conduction, various influencing dipoles and their orientations, the direction of spread, changes in the direction of tracts, changes in resistance of surrounding tissue, etc. What happens is a response is near-field (like P37), far-field (like P31) or both (like Wave I and N13/P13).
Bonus Material: Here’s a video to demonstrate the formation of a wave. You’ll see how the orientation of your recording electrodes to the electric current makes a difference in the waveform you get. And this electric current from the heart in the video, but still the same principal.
Keep Learning
Here are some related guides and posts that you might enjoy next.

How To Have Deep Dive Neuromonitoring Conversations That Pays Off…
How To Have A Neuromonitoring Discussion One of the reasons for starting this website was to make sure I was part of the neuromonitoring conversation. It was a decision I made early in my career... and I'm glad I did. Hearing the different perspectives and experiences...

Intraoperative EMG: Referential or Bipolar?
Recording Electrodes For EMG in the Operating Room: Referential or Bipolar? If your IONM manager walked into the OR in the middle of your case, took a look at your intraoperative EMG traces and started questioning your setup, could you defend yourself? I try to do...

BAER During MVD Surgery: A New Protocol?
BAER (Brainstem Auditory Evoked Potentials) During Microvascular Decompression Surgery You might remember when I was complaining about using ABR in the operating room and how to adjust the click polarity to help obtain a more reliable BAER. But my first gripe, having...
Bye-Bye Neuromonitoring Forum
Goodbye To The Neuromonitoring Forum One area of the website that I thought had the most potential to be an asset for the IONM community was the neuromonitoring forum. But it has been several months now and it is still a complete ghost town. I'm honestly not too...

EMG Nerve Monitoring During Minimally Invasive Fusion of the Sacroiliac Joint
Minimally Invasive Fusion of the Sacroiliac Joint Using EMG Nerve Monitoring EMG nerve monitoring in lumbar surgery makes up a large percentage of cases monitored every year. Using EMG nerve monitoring during SI joint fusions seems to be less utilized, even though the...

Physical Exam Scope Of Practice For The Surgical Neurophysiologist
SNP's Performing A Physical Exam: Who Should Do It And Who Shouldn't... Before any case is monitored, all pertinent patient history, signs, symptoms, physical exam findings and diagnostics should be gathered, documented and relayed to any oversight physician that may...

Hi
I am planning to go for October CNIM test. Is the course you are offering in 126 days? Or earlier?
What study mayerial do you recommend?
What is the neuroanatomy study guide for CNIM test? Neuroanatomy is huge.
Thank you
Sophie
As of this date, the site is under a redesign and I am still getting things up and going again. The timer that you see there is a default to start at the beginning of the new year. That probably won’t be the start date. Please check back after the site has been relaunched.