
Surgical Neurophysiologist or Medical Doctor?
There seems to be more than a handful of people that want to go to medical school but decided to get into intraoperative neuromonitoring in the meantime. Others are on the fence as to where they should take their career while still in school. I’m more than happy to lend advice but will try to keep any emotional factor out of it.
I’ve had similar discussions with my niece as it pertains to nursing school, PA school and medical school. So I’ll give similar advice and relate it to neuromonitoring, but you should be made aware of the following caveats:
- This is going to be completely financial advice. This is by no means the only or main factor to consider, but you really should play with the numbers to understand what you’re getting into whatever route you take. I can’t help you on the quality of life side. I have no idea what’s going to bring joy to your life or make you want to rip your hair out. You’ll have to tip the scales one way or another in that respect.
- The numbers that I’m going to use are best guesses… but they stink. These are assumed averages that span a large range with many unpredictable factors in play, including income, years to earn income, inflation/deflation, interest rate on loans, rate of return on investments, consistency of current tax structure and where one might fall from year to year (single/married, # of dependents), discipline to pay off debt and/or invest earnings, reimbursement rates for services rendered, hours worked per week, scholarships earned, etc. Instead of telling me how far off my numbers are in your experience, just change them in your calculator and come up with your own assumptions. Chances are neither of us will be completely right.
- You can use these numbers to apply it to other areas of interest, like research, audiology, chiropractic, nursing, PA school, etc.
- Talk with medical doctors for their advice on entering their field. I’m familiar with their workload but have no first-hand experience. Many have become sour to their field of choice. Find out why and try to make educated assumptions if it is really a problem or a problem of “the grass is always greener.”
Cost Of Medical School
The first thing we need to really look at is that overwhelming amount of debt obtained by a medical doctor. For 2017, the median 4-year cost of medical school is $240,000 for public school and $314,000 for private school. DO school is in the same ballpark. That’s crazy considering medical school cost only $13,5000 (or close to $50,000 in today’s dollars) in 1978.
Even with grants and scholarships chipping away at that debt, interest rates can accumulate for some of the loans taken out by most students up to 25% of the loan during their residency. A rough estimate of $212,500 was given here after considering both money earned towards the cost of school and interest accrued on the loans during residency. It’s tough to figure the interest rate used there since we don’t know what portion of the loan is accumulating interest or how long the residency will last, but it’s probably between 6-10% using those numbers. I’m not sure what loans are currently at, but that seems like a pretty high rate, so I might be a little over on that side of the cost.
Lost Wages
Getting through medical school and residency takes a very long time, and some specialties might be looking at a decade of training. That’s great for the public but not so great on the young doctor’s pocketbook. But we know that they’ve got to at least get through 4 years of school.
Neuromonitoring salaries start off pretty low, but can have a nice jump early on in your career when you 1) start doing cases on your own 2) pass the CNIM. While you might expect to make something like $45,000 the first year in training, the earning potential of someone in the 4th year is probably close to $70,000. Where did I get that number? There’s an old ASET survey, looking at ranges given by other websites and what I’ve seen or heard. Could be higher. Could be lower. But it seemed reasonable, maybe a little conservative.
So we’ll call it $235,000 the SNP earns over the 4 year period at an effective tax rate of 20% leaves us at $188,000 of cash you can spend.
Add the $212,500 (the debt) + 188,000 (the opportunity cost) and you get the medical student down $400,500 in the first four years (not including any money made on investments in the opportunity cost).
Since residents earn about $40,000-$50,000 in residency, the difference in income for those years is less severe for the medical student. So the final number is probably closer to $450,000 in the hole.
But there is one MAJOR factor that I did not account for, which you should. And that’s the amount of hours you’ll put into medical school and residency. You’re looking at 60-80 hour work weeks, and that really inflates the opportunity cost. Here’s a nice image that breaks that down even further at a lower per dollar rate than I estimated.
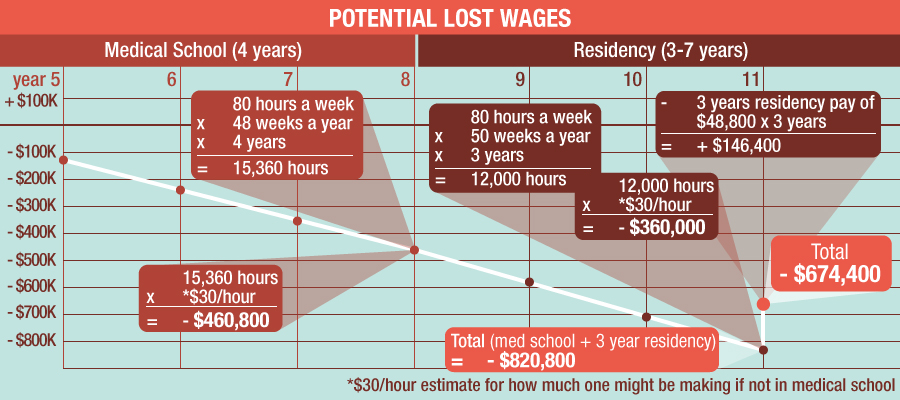
“The $1 million Dollar Mistake”
That’s the sensationalized headline of the referenced article. They’ve come up with very similar numbers but took it a step further to show the consequences of carrying that financial burden all the way to the maturity of a 30-year loan at 7.5% added to their debt. Not quite a million, probably a higher interest rate than what’s available and assuming poor money management by the physician, but the point is should be well taken that there is a hole to dig out of should you chose to go into medicine.
But there are 2 real saving graces for the medical physician. First is that there are jobs available, so you can pretty much count on the fact that you’re not earning a worthless degree. Second is that a lot of the specialties pay really, really well.
For most specialties, the new medical doctor should be able to stop their financial hemorrhage by paying off their debt at an accelerated rate. If I were in their shoes, I’d try to get it done in no more than 5 years. According to the AAMC, the typical repayment period for medical doctors is 10 years, which comes out to about $328,000 total on $176,000 loans and 3 years of residency (which was a little lower of a starting point that what I figured above). Considering that the average age of graduation is 24, it seems like most medical physicians are getting rid of their loans around age 36-37.
Earned Wages
Here’s a nice layout for those interested in the amount of earnings vs worked hours for different specialties within the medical field.
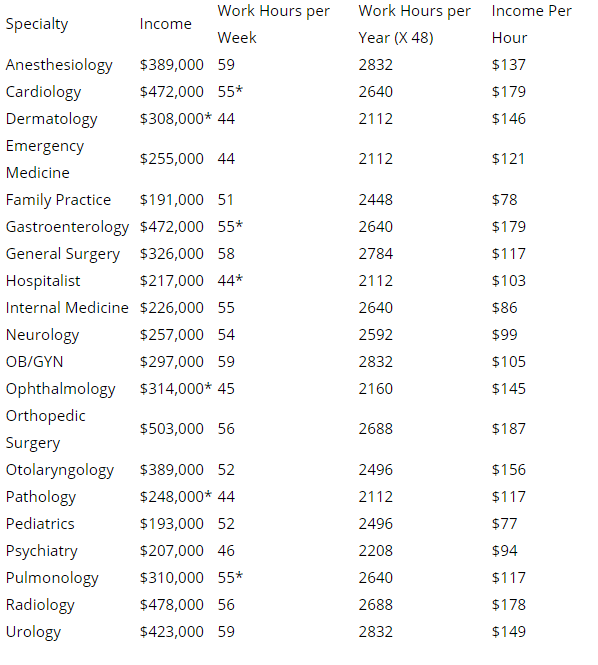
Seems like all medical staff is working long hours, but most are still making a killing per hour. I know there are some workhorses out there that have similar hours worked in the neuromonitoring space, but over the peaks and valleys of the year, most fall right around 42 hours on average.
But there are some MDs that are creeping closer to what a neuromonitoring clinician would make. Those same doctors would also find it more difficult to pay off the student loan debt before it snowballs a bit.
So it’s probably a good idea to take a look at some comparisons.
Using this tax calculator and my home state of Florida (no state tax), here are some rough estimates:
SNP = $70,000. Take home pay $54,000.
Lowest MD earner = $191,000. Take home pay of $137,000.
That’s a difference of $83,000 earned per year. That would take only 5.4 years to reach the break-even (probably more like 6 when interest rates on loans still accumulating). But remember that they are working 9 hours more per week, or 468 hours per year. That’s like cramming another 11.7 weeks or 3 months of work into each year.
Highest earner = $503,000. Take home pay of $333,000.
That’s a difference of $279,000 earned per year. That would take only 1.6 years to reach the break-even. But remember that they are working 14 hours more per week, 728 hours per year. That’s like cramming another 14 weeks or 3.5 months of work into each year.
So it seems clear that even though the chips are stacked against them, a medical doctor can rapidly catch up and set themselves up nicely going forward (financially speaking).
What About Testing The Waters?
It would make sense to test out neuromonitoring before medical school, and I know a couple of people that have gone that route. But when you look at the numbers above, this decision starts to weigh more heavily on an emotional justification over a financial one. But you might see it in the same light as buying an insurance policy.
It would be great if you could go to medical school and work this as a part time or per diem gig. But knowing the unpredictability of our schedule and the unrelenting schedule of a medical student, I doubt this ends up working well for most. If you’re a bright student and don’t want to go after any competitive specialty, maybe it can work out. But I would say that the person that lets their grades slip and can’t compete for a higher paying specialty are making a huge mistake. In some cases the difference between what you earned monitoring cases could be earned back in a couple years.
But all that might just be pie in the sky. It’s hard enough finding your first neuromonitoring job, but trying to find one for a couple years only really limits your options. Because of the cost incurred by the company or hospital to train you the first year is so high, you might find yourself on the hook to pay that back should you decide to leave before the stipulated time. If your plan was just to work for a year or two, you might find it hard to impossible to find something that works out for you.
My conclusion
This thing could go either way.
If you’re as willing to put in the work in IONM as someone has to do to get through medical school, you’re going to earn a lot more than the $70,000 quoted. That’s on bonus money and most likely raises as you’re an asset worth paying for. If you’re smart and lucky with the money you’ve earned, that break-even point is going to extend much further out than what’s seen above.
If you’re smart about going to in an in-state medical school to keep cost low, choose a specialty that earns more money and continue to live like a resident for 5-10 years after residency to pay off your loans and invest, start medical school before age 35, you’re going to most likely live a very financially stable life as a reward for your hard work. Accept that you’re taking on a huge risk with all that student loan debt and long hours, but the payoff is worth it. Play it conservative and you’ll reap the rewards.
But the main takeaway I hope most people take away from this article is this:
- Whichever route you take, be aware of the smartest route to get you there. It can mean hundreds of thousands of dollars to you over your working career.
- Do not let money be the only factor. Look at the quality of life and interest in the field you’re choosing. You’re going to be spending 40-60 hours per week doing it. Make sure you’re enjoying yourself.
- Look at other factors like the risk of a lawsuit, stability of the career, respect of the position, your risk tolerance for making life and death choices for other people, etc.

Joe Hartman
Subscribe to our Awesome Newsletter.
Keep Learning
Here are some related guides and posts that you might enjoy next.

How To Have Deep Dive Neuromonitoring Conversations That Pays Off…
How To Have A Neuromonitoring Discussion One of the reasons for starting this website was to make sure I was part of the neuromonitoring conversation. It was a decision I made early in my career... and I'm glad I did. Hearing the different perspectives and experiences...

Intraoperative EMG: Referential or Bipolar?
Recording Electrodes For EMG in the Operating Room: Referential or Bipolar? If your IONM manager walked into the OR in the middle of your case, took a look at your intraoperative EMG traces and started questioning your setup, could you defend yourself? I try to do...

BAER During MVD Surgery: A New Protocol?
BAER (Brainstem Auditory Evoked Potentials) During Microvascular Decompression Surgery You might remember when I was complaining about using ABR in the operating room and how to adjust the click polarity to help obtain a more reliable BAER. But my first gripe, having...
Bye-Bye Neuromonitoring Forum
Goodbye To The Neuromonitoring Forum One area of the website that I thought had the most potential to be an asset for the IONM community was the neuromonitoring forum. But it has been several months now and it is still a complete ghost town. I'm honestly not too...

EMG Nerve Monitoring During Minimally Invasive Fusion of the Sacroiliac Joint
Minimally Invasive Fusion of the Sacroiliac Joint Using EMG Nerve Monitoring EMG nerve monitoring in lumbar surgery makes up a large percentage of cases monitored every year. Using EMG nerve monitoring during SI joint fusions seems to be less utilized, even though the...

Physical Exam Scope Of Practice For The Surgical Neurophysiologist
SNP's Performing A Physical Exam: Who Should Do It And Who Shouldn't... Before any case is monitored, all pertinent patient history, signs, symptoms, physical exam findings and diagnostics should be gathered, documented and relayed to any oversight physician that may...

0 Comments