Somatosensory Evoked Potential Test Variability
In my previous 2 post about temporal dispersion and somatosensory evoked potential test variability, I went over how to ID trial-to-trial variability, how to handle it and what was happening to the waveform. I’m going to add a little more to the conversation and try sum up my thoughts.
Variability… What’s Happened Here?
There’s plenty of culprits to point the finger at, with advanced age and poorly regulated blood sugar levels being at the top of the list.
According to Lascelles and Thomas, 1966 and Toghi, 1977, the following happens to nerves as we age:
- increase loss of large fibers
- increase incidence of fibers with segmental demyelination
- shortening of the internodal segment
And Chopra 1969 looked at the nerve integrity of diabetics vs. other control groups and found…
Loss of myelinated nerve fibers of all sizes were observed in diabetic patients compared to controls. Loss of the large diameter fibers was severe in some of the diabetics with neuropathy.
But even though I keep coming back to age and diabetes, there’s plenty of other things to mess up your nerves. Alcohol, thyroid disorders, autoimmune, etc.
And beyond looking directly at what’s happened to the nerve, here’s something I found interesting as a possible additive problem …
Meissner corpuscles on the fingers decreases 4X from the ages of 12 to 50. The rate at which they are lost correlates well with the age-related loss in touch sensitivity for small probes (Thornbury and Mistretta, 1981).
So the population of receptors, which drive neural activity and promote cellular early immediate gene responses are also decreasing. If you don’t use it, you lose it.
Now don’t let what I saying here confuse things even more. When we elicit a somatosensory evoked potential, test are run by directly stimulating the nerve. This bypasses the receptors. So receptor drop off does not affect the SSEP level of excitation directly. But since the evoked response travels along the nerve fibers that naturally conduct touch/vibration, we may be able to expect a drop off in nerve function as the receptors drop off with age. Just something I thought I’d mention that other chiro neuro’s might appreciate.
There Might Be More To Variable SSEP Than Peripheral Nerve Problems
There’s quite a long way to travel from the distal limbs to the cortex in order to record a SSEP. There can be problems at many different places along the way. Especially in our patient population. I mean, they’re all surgical candidate, right?
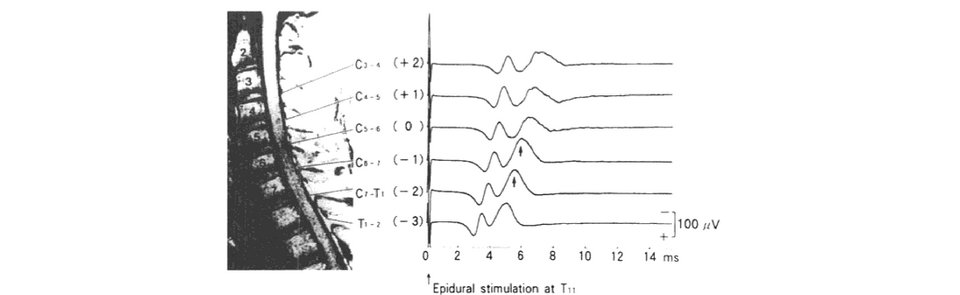
Studies done by Tani, 2002 demonstrated changes in SSEP when there was partial or complete conduction block in the cervical spine.
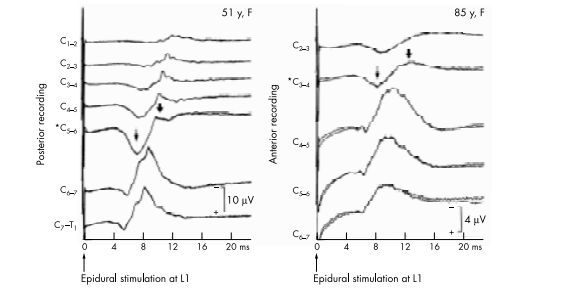
Conduction block SSEP
They showed incremental electrophysiological studies can identify the site of conduction block by showing an abrupt reduction in size of the negative peak accompanied by an enlargement of the initial positive peak.
At this site, a blocked fibre contributes a normal positivity followed by a substantially reduced negativity, as the impulse approaches without reaching the recording site. This reduction in negativity not only decreases the negative peak of the evoked potential but also increases its positive peak resulting from loss of physiological phase cancellation. Rostral to a conduction block, a blocked fibre gives rise to a killed end effect with a volume conducted positive wave. Thus monophasic positive evoked potentials rostrally are characteristic of complete focal conduction block.
While they’ve used these types of studies to demonstrate that elderly patients typically have conduction block from myelopathy in upper cervical lesions (opposed to middle cervical in younger patients), as well using this test in order to pinpoint the area of compression and limit the surgical levels, you can see that there are changes to the SSEP potentials as it crosses the area of myelopathy. There is clearly changes in the signal once traveling past that conduction block.
Summing Things Up
Increases in temporal dispersion, resulting in prolonged latency, longer duration, more components and smaller amplitude size, cause less than optimal responses and can be difficult to impossible to record in an electrically harsh operating room. There are many causes of the same problem seen on somatosensory evoked potential test, and multiple problems can be seen in the same patient (the elderly diabetic with cord compression).
As our patient population continues to get older and sicker, keeping your impedance low, recording as near-field as possible and working to eliminate noise in all channels is even more important in these patients susceptible poor signal-to-noise potentials.
Keep Learning
Here are some related guides and posts that you might enjoy next.

How To Have Deep Dive Neuromonitoring Conversations That Pays Off…
How To Have A Neuromonitoring Discussion One of the reasons for starting this website was to make sure I was part of the neuromonitoring conversation. It was a decision I made early in my career... and I'm glad I did. Hearing the different perspectives and experiences...

Intraoperative EMG: Referential or Bipolar?
Recording Electrodes For EMG in the Operating Room: Referential or Bipolar? If your IONM manager walked into the OR in the middle of your case, took a look at your intraoperative EMG traces and started questioning your setup, could you defend yourself? I try to do...

BAER During MVD Surgery: A New Protocol?
BAER (Brainstem Auditory Evoked Potentials) During Microvascular Decompression Surgery You might remember when I was complaining about using ABR in the operating room and how to adjust the click polarity to help obtain a more reliable BAER. But my first gripe, having...
Bye-Bye Neuromonitoring Forum
Goodbye To The Neuromonitoring Forum One area of the website that I thought had the most potential to be an asset for the IONM community was the neuromonitoring forum. But it has been several months now and it is still a complete ghost town. I'm honestly not too...

EMG Nerve Monitoring During Minimally Invasive Fusion of the Sacroiliac Joint
Minimally Invasive Fusion of the Sacroiliac Joint Using EMG Nerve Monitoring EMG nerve monitoring in lumbar surgery makes up a large percentage of cases monitored every year. Using EMG nerve monitoring during SI joint fusions seems to be less utilized, even though the...

Physical Exam Scope Of Practice For The Surgical Neurophysiologist
SNP's Performing A Physical Exam: Who Should Do It And Who Shouldn't... Before any case is monitored, all pertinent patient history, signs, symptoms, physical exam findings and diagnostics should be gathered, documented and relayed to any oversight physician that may...
