Brainstem Auditory Evoked Potential Used To Predict The Need For Duraplasty In Chiari Malformation Type I Decompression
Have you ever had the following conversation with a surgeon after decompression is complete?
Surgeon: How do things looks (refering to SSEP and/or BAEP)?
Neurophysiologist: Everything looks good.
Surgeon: Did it get better? We just decompressed the hell out of that thing.
Neurophysiologist: No, we’re trending right at baseline.
Surgeon: Oh. (pouty face under the mask)

Image from healthwise-everythinghealth.blogspot.com
If you’ve done more than 100 cases, I’m sure you’ve been asked that question at least once. And the answer is almost always “no improvement.” And almost as often as you give that answer, it really has no importance clinically.
All you really want to know is if there was a significant change indicating possible injury. Outside of repair on an acute injury, the safe bet is not to even try to use BAEP or SSEP to predict surgical improvement.
There may be an exception. According to two papers (J Neurosurg. 2003 Mar;98(3):459-64 and J Clin Neurophysiol. 2009 Apr;26(2):70-5), using improvement in central conduction time of brainstem auditory evoked potential (time difference between wave I and wave V) may have identified that most of the neurological improvement, as a result of a posterior fossa decompression during Arnold Chiari malformation, happens as a result of bone decompression and division of the atlantooccipital membrane, rather than after opening of the dura.

Image from Zamel study linked above
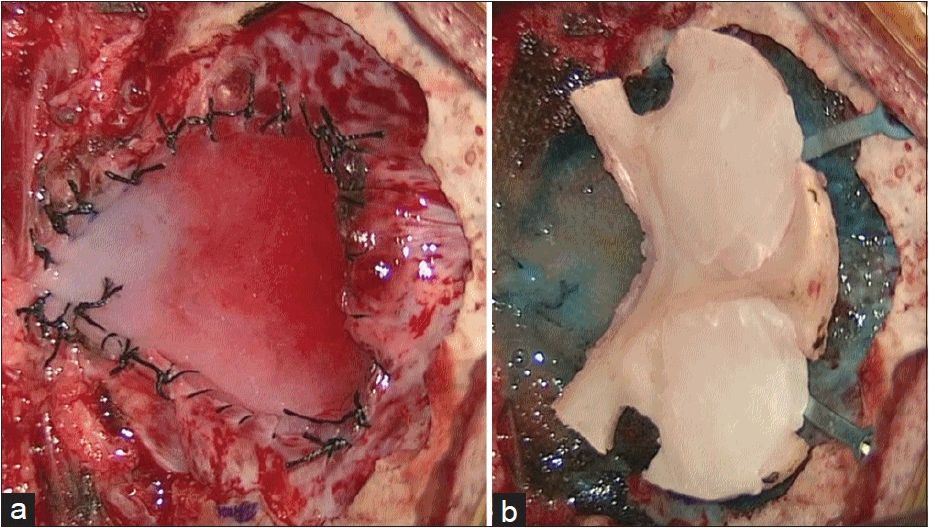
In Anderson’s study, the postop complication rate was 42% for those with the duraplasty, while it was only 10% in those without duraplasty. There was no significant difference in improvement rates between the two groups. Their correlation may help pique the interest in other surgeons to limit the amount of duraplasty performed, and most likely reduce neurological compromise. While more studies are needed to validate or disprove these studies, it is an interesting finding.
What does that mean for you?
I don’t think that brainstem auditory evoked potential should be performed on the sole basis of looking for improvement and telling the surgeon that they should or shouldn’t do a duraplasty. I’m not even so certain that BAEP is the best idea for monitoring Arnold-Chiari malformation (though you may find it as a useful adjunct to SSEP). But if you are running BAEP during decompression of Chiari malformation, you should be aware of it. And you should make sure the surgeon is aware as well.
UPDATE 8-11-16: It has been a couple years since I put out this post, and my opinion has changed… some. I’ve got another 10 of these cases under my belt now after working with another surgeon using this criterion. This time around, I also incorporated SSEP. For the recording channels, I used EP, a cervical, 2 far-field subcortical and 2 cortical channels to also look for a reduction in latency. The responses ranged from abrupt BAER signal changes, changes that happened in the BAER first and then SSEP, in SSEP only and no changes at all.
This surgeon is lightning quick, so there wasn’t a lot of time in between the start of bony decompression and completion. Because these are usually done on kids, data acquisition was pretty fast, so I was able to move through the different modalities without needing to average too much.
One other important piece to note is that this surgeon did not use our signals as an all-or-none reason to perform duraplasty. He would let me know that even if I did see a change on BAEP or SSEP, he was planning on doing it anyways due to other factors.
So I have come around on the fact that this long-standing compression can have an immediate change in latency on bony decompression, which isn’t what I’ve noticed in myelopathic spine cases at the same frequency.
I would now like to see outcome measures of a group that never gets duraplasty, ones that always get duraplasty and ones that get selective duraplasty and see what the results give us. That is where we can see the clinical utility of brainstem evoked potentials for Arnold Chiari decompression surgery. But in till that time, the literature does seem to suggest that this technique may hold value in the surgeon’s reasoning to perform a duraplasty.
Keep Learning
Here are some related guides and posts that you might enjoy next.

How To Have Deep Dive Neuromonitoring Conversations That Pays Off…
How To Have A Neuromonitoring Discussion One of the reasons for starting this website was to make sure I was part of the neuromonitoring conversation. It was a decision I made early in my career... and I'm glad I did. Hearing the different perspectives and experiences...

Intraoperative EMG: Referential or Bipolar?
Recording Electrodes For EMG in the Operating Room: Referential or Bipolar? If your IONM manager walked into the OR in the middle of your case, took a look at your intraoperative EMG traces and started questioning your setup, could you defend yourself? I try to do...

BAER During MVD Surgery: A New Protocol?
BAER (Brainstem Auditory Evoked Potentials) During Microvascular Decompression Surgery You might remember when I was complaining about using ABR in the operating room and how to adjust the click polarity to help obtain a more reliable BAER. But my first gripe, having...
Bye-Bye Neuromonitoring Forum
Goodbye To The Neuromonitoring Forum One area of the website that I thought had the most potential to be an asset for the IONM community was the neuromonitoring forum. But it has been several months now and it is still a complete ghost town. I'm honestly not too...

EMG Nerve Monitoring During Minimally Invasive Fusion of the Sacroiliac Joint
Minimally Invasive Fusion of the Sacroiliac Joint Using EMG Nerve Monitoring EMG nerve monitoring in lumbar surgery makes up a large percentage of cases monitored every year. Using EMG nerve monitoring during SI joint fusions seems to be less utilized, even though the...

Physical Exam Scope Of Practice For The Surgical Neurophysiologist
SNP's Performing A Physical Exam: Who Should Do It And Who Shouldn't... Before any case is monitored, all pertinent patient history, signs, symptoms, physical exam findings and diagnostics should be gathered, documented and relayed to any oversight physician that may...
