How Resourceful Of A Neuromonitoring Tech Are You?
First off, let me start this topic off by saying that I’m not a big fan of the term neuromonitoring tech (I prefer surgical neurophysiologist or SNP). But I really want to address those in the field that might embrace the title of neuromonitoring tech. This person might feel that they are there to set the patient up as prescribed by their company’s policy and procedures. Any changes that need to be made is out of their job description.
That’s not the role of anyone doing neuromonitoring, no matter what you call yourself.
You need to understand what you’re doing, why you’re doing it and when to make changes. You need to be flexible, thoughtful and thorough.
I started off under the tutelage of Joe Danto and systemization of his techniques by Joe Conlon. Joe Danto knows this field like few do. He started his career at a time when adapting due to limitations was necessary in order to get things done. And he was an absolute Maguyver in the OR. Grab 20 yellow wires, slice it, dice it, tape it back together and get beautiful responses.
But having to adapt due to limitations of equipment started to become less of a problem. In comes Joe Conlon and does what he does… makes the difficult easy. With systems in place, he was able to eliminate certain problems and know where to go next if things aren’t as they should be.
I think most groups have adopted their protocols in order to give the neuromonitoring tech the best starting place – most of the time. And I absolutely agree that this should be the way things are done. One of my jobs is to look over current policies and to make sure that they are what is currently considered best practices.
But we shouldn’t devalue the ability of a neuromonitoring tech to adapt. And since a good percentage of oversight physicians spend much less time in the OR compared to the neuromonitoring tech, they may not be the go-to person to ask those types of questions.
One Of Your Tools – The Reference Jumper Cable
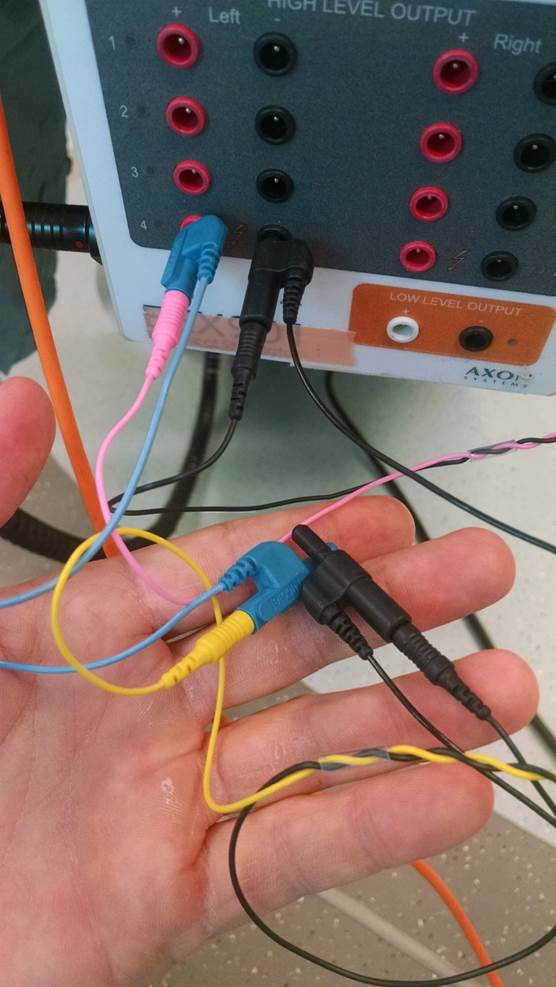
You can see the jumper reference cable here (blue and black)
There are plenty of neuromonitoring techs that have gone rummaging through their bags looking for their last green wire to use as the ground and found this (usually) black, double-headed cable and thought to themselves – “what’s with this thingy?”
That thingy (the jumper reference cable) is a nice addition to anyone’s bag. I’d actually request 2 if I were you. I’ve used these a number of times to get me out of a pinch. They don’t always make their way out of my bag, but I do make sure that I have them available in every case.
For the sake of those less familiar, let’s go over some scenarios where the neuromonitoring tech might make use of these in order to better adapt to the case at hand. I’m not going to give every use that I can think of. I’d like to see what else the community can come up with. But here are a few:
- If you’ve used an older version of the Cadwell MEP box (CV-2), then you’ve used the jumper in order to be able to simulate the right and left cortex using the same 2 electrodes.
- Using tripolar J-hook electrodes for stimulating a peripheral nerve, you can place both your anodes into the jumper cable and then to your box.
- If you’re low on electrodes and plan on doing referential recording EMGs, you can save yourself an electrode. For instance, say your monitoring abdominal muscles. Instead of using 4 electrodes, you could use 3 total. 1 in the upper and 1 in the lower. The 1 electrode in the middle abs can be linked to both the upper and lower.
- You could link M1-M2 and M3-M4 to cover a greater area of stimulation for tcMEP (as far as I know, those doing this technique have yet to publish their findings that you can get threshold at a lower output of electrical current).
There’re 4 ideas on how to adapt your setup using these reference jumper cables. Does anyone else have an example they’d like to share to help make a neuromonitoring tech into a surgical neurophysiologist?

Joe Hartman
Subscribe to our Awesome Newsletter.
2 Comments
Keep Learning
Here are some related guides and posts that you might enjoy next.

How To Have Deep Dive Neuromonitoring Conversations That Pays Off…
How To Have A Neuromonitoring Discussion One of the reasons for starting this website was to make sure I was part of the neuromonitoring conversation. It was a decision I made early in my career... and I'm glad I did. Hearing the different perspectives and experiences...

Intraoperative EMG: Referential or Bipolar?
Recording Electrodes For EMG in the Operating Room: Referential or Bipolar? If your IONM manager walked into the OR in the middle of your case, took a look at your intraoperative EMG traces and started questioning your setup, could you defend yourself? I try to do...

BAER During MVD Surgery: A New Protocol?
BAER (Brainstem Auditory Evoked Potentials) During Microvascular Decompression Surgery You might remember when I was complaining about using ABR in the operating room and how to adjust the click polarity to help obtain a more reliable BAER. But my first gripe, having...
Bye-Bye Neuromonitoring Forum
Goodbye To The Neuromonitoring Forum One area of the website that I thought had the most potential to be an asset for the IONM community was the neuromonitoring forum. But it has been several months now and it is still a complete ghost town. I'm honestly not too...

EMG Nerve Monitoring During Minimally Invasive Fusion of the Sacroiliac Joint
Minimally Invasive Fusion of the Sacroiliac Joint Using EMG Nerve Monitoring EMG nerve monitoring in lumbar surgery makes up a large percentage of cases monitored every year. Using EMG nerve monitoring during SI joint fusions seems to be less utilized, even though the...

Physical Exam Scope Of Practice For The Surgical Neurophysiologist
SNP's Performing A Physical Exam: Who Should Do It And Who Shouldn't... Before any case is monitored, all pertinent patient history, signs, symptoms, physical exam findings and diagnostics should be gathered, documented and relayed to any oversight physician that may...

Ah, the humble little jumper cable (I’m not sure how the word ‘reference’ got in there) an unsung hero of the OR. It has nearly faded into history. While is still useful at times for stimulation, re-configurable input montages have rendered them nearly useless on the recording side. Your example #3 could be accomplished more easily by reallocating the single input pin to two different channels. This would also avoid one of the biggest problems with jumpers, the additional noise introduce because of the extra connection. There is also one situation that you should not use the jumper. I’ve seen people using 32 channel systems with two separate 16 channel amplifiers use a jumper to connect the grounds of both amplifiers to a single electrode. First of all, the ground for each amplifier should be positioned in order to maximize the CMRR. Secondly, the jumper could allow internal noise from one amplifier to contaminate signals in the other,
Unsung hero indeed, Andrew Goldstein!
The jumper cable has long been my go-to accessory for tcMEP stimulation in cranial cases where hemispheric isolation is required but not obtainable using only M1/M2 leads.
How frustrating is it, during an aneurysm clipping/coiling, tumor resection, or even a carotid endarterectomy, to run baseline MEPs from M1/M2, only to get crossover responses from the contralateral side of interest?
Used in conjunction with a multi-channel MEP stimulator, i.e. Cadwell’s TCS-4, and just one extra electrode placed at midline – my placement preference is between Fz and Cz (FCz?) – the handy little jumper can be used to create either an M1 or M2 – FCz montage, depending on the hemisphere at risk.
Hemispherically isolated MEP responses increase the likelihood that stimulation is not spreading to deeper motor tracts, thus allowing the responses evoked to be highly sensitive to the actual cranial area at risk.
It’s been my experience that in cases where the use of M1/M2 results in crossover responses, utilizing the jumper cable to create alternate montages results in hemispheric isolation many more times than not, giving me confidence that I’m contributing to the safest surgical or endovascular experience possible for the patients I monitor. I keep no less than 2 jumpers in my IOM toolbox at all times!